

Patellofemoral Joint Replacement
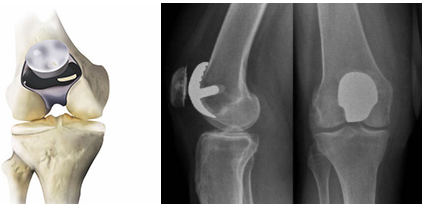
Patellofemoral replacement, often called knee cap replacement or patellofemoral arthroplasty, is a type of partial knee replacement. In this procedure the arthritic surface of patella (knee cap) is replaced with highly cross linked polyethylene and the corresponding articular surface on distal femur is replaced with metal cap. The healthy cartilage and bone, as well as all of the ligaments in the rest of the knee, are preserved. This is ideal procedure for patients with isolated patellofemoral joint arthritis, considering the rest of knee joint is normal. Most of these patients are young and often suggested to wait for total knee replacement till they are in their fifties or sixties despite the pain and disabilities of bone on bone arthritis.
Anatomy
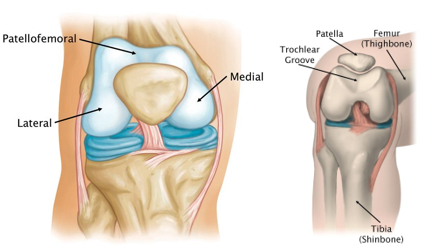
Knee is divided into three major compartments:
- Medial compartment - the inside part of the knee
- Lateral compartment - the outside part of the knee
- Patellofemoral compartment - the front of the knee between the patella (kneecap) and femur.
Within the patellofemoral compartment, the patella lies in a groove on the top of the femur called the trochlea. When you bend or straighten your knee, the patella moves back and forth inside this trochlear groove. Articular cartilage covers the ends of the femur, trochlear groove, and the under surface of the patella. This articular cartilage allows pain free, smooth movements of the joint
Patellofemoral Arthritis
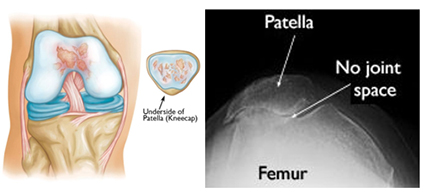
In patellofemoral arthritis, the cartilage protecting the undersurface of knee cap and /or femoral trochlea wears away. As the cartilage wears away, it becomes frayed and the underlying bone may become exposed. Thus the making the joint stiff and movements painful. Patellofemoral joint arthritis occurs in isolation in approximately 10% of patients with arthritis of the knee. The patients tend to be younger, with a preponderance of females.
Symptoms
Patients with patellofemoral arthritis often present with symptoms of anterior knee pain that is worse with climbing stairs, getting up from sitting position and sitting for prolonged periods of time. Patients may also likely experience a crunching or grinding sensation when doing stairs or standing from a seated position. Patient can also have restricted knee range of motion.
Indications of patellofemoral joint arthroplasty
- Advanced isolated primary patellofemoral joint arthritis (Bone on bone arthritis)
- Patellofemoral arthritis with trochlear dysplasia, often with a history of instability
- Post-traumatic PF arthritis
Ideal Patient for patellofemoral joint replacement
The ideal patient for PFJ replacement is one with severe signs and symptoms of isolated patellofemoral disease. These correlate with radiologically proven arthritis, best demonstrated on tangential views of the patellofemoral joint. These patients usually have:
- Minimal pain while walking on level surfaces
- Isolated anterior retropatellar pain that is exacerbated by:
- Standing from seated position
- Climbing up/down stairs
- Walking on uneven surfaces
- Sitting long periods with knee flexed
Advantages of patellofemoral joint replacement
The major advantage over a total knee replacement is that the knee will have a much more natural feel to it. This is because all the ligaments in the knee are preserved along with rest of normal articular cartilage. Also the functional and activity scores are better when compared to total knee replacement. Other than this the procedure is somewhat smaller, so discharge from hospital is a day or two earlier, recovery a little quicker and aim to return to work / activities sooner than with a total knee replacement.
Procedure
The surgery is performed under spinal or general anaesthesia combined with intraoperative injections of local anaesthesia, and a "Pain buster" local anaesthetic catheter which is left in the joint. In addition to this, Femoral Nerve blocks or regional anaesthesia is also added.
We perform diagnostic knee arthroscopy for all the patients before the actual skin incision to confirm the suitability of the patient for the procedure. Patient undergoes patellofemoral arthroplasty only if he has isolated patellofemoral arthritis and rest of the knee is considerably normal.
An incision is made around the front of the knee, exposing the distal femur and patella. The incision is considerably smaller than the incision of total knee replacement. Specialized surgical guides are used to remove the worn-out surface and shape the end of the femur. The metal component, similar in size and shape to the end of the femur, is cemented to the bone. Patella is everted and damaged cartilage along with some bone is shaved off from it’s the inner surface and the patellar button is cement on it.
Once the components are inserted, the knee is moved along the range of motion to confirm the accurate positioning of the implant. The wound is closed with absorbable sutures with pain buster and suction drain in situ. The operation takes about 45 minutes to complete. We use Zimmer® Gender Solutions™ Patello-Femoral Joint (PFJ) System for this surgery.

Post operative care
- The surgery takes about 1.5 hours to complete.
- You will be transferred from the operating room to the recovery unit.
- In recovery, you will be observed and given any pain relief you require. You will stay in the recovery room until you recover from the anaesthetic. I.e. you will be arousable, comfortable and your observations stable.
- This time varies from patient to patient.
- Once comfortable you will be transferred to the second stage recovery unit.
- You will be given something light to eat and drink.
- You will notice that you have a large dressing on your operated leg. This dressing extends from your thigh to your ankle.
- There will also be a knee immobilizer (splint) in place over the dressing.
- Under the dressing and resting in the wound, you will have the local anaesthetic catheter and pump along with the suction drain. Both these tubes along with the bulky dressing come out on day 3.
- Once comfortable you will be transferred to the orthopedic ward.
- Physiotherapist will see you next day morning and get you up and will make you walk with the help of walking frame and also go through with the exercises.
- You will need to use the knee splint while walking for first few days, till you can lift your leg straight up in the bed (Active straight leg raise).
- Physiotherapist will help you to progress from walking frame to crutches and then to walking stick.
Discharge from hospital
- You will be discharged from hospital on day 3. The bulky dressing and all the tubes will come out before you go home.
- A waterproof dressing will be in place, which will stay in place for next 2 weeks.
- You will be given medication to take home and it is very important to take this medication as prescribed.
- You will be given an appointment to see your surgeon after 2 weeks from your surgery.
General information
- Bruising around the thigh/knee area is not uncommon and may be a result of the tourniquet used during the surgery. It may extend down the leg as far as the foot. It usually resolved within 10 to 14 days.
- Some swelling and warmth should be expected following surgery.
- If you develop increased redness, swelling or fever, call us or after hours, the hospital or your local doctor.
General expectations
These are averages, each case is individualised by your general health, age and attitude.
- For approximately 2 weeks after surgery, your activity level is usually limited, however you will be able to walk independently and use bathroom and kitchen facilities.
- After 2 weeks, you will be able to engage in moderate activities such as driving a car and climbing stairs.
- Within 6 weeks you will have resumed most of your normal activities. Squatting and kneeling come with time.
- Complete surgical healing takes 6 to 8 weeks. During this time, some swelling and discomfort is normal and should be manageable with the prescribed medications.
- After this time the knee tissues start to begin to soften and become more natural.
- Some patients may require an injection of cortisone (after 12 weeks) to relieve tissue soreness due to surgery and readjustment of the knee.
- Some patients may experience a small area of numbness on the lateral aspect (outside edge) of the incision. This may or may not resolve over time and can take 6 to 12 months.
Exercises to be done
- To reduce stiffness and obtain maximum function of your knee, it is important to maintain a good balance of rest and exercise.
- Listen to your body; too much activity will produce increased swelling and/or pain; too little activity could prolong your recovery and/or limit your knee mobility.
- Generally walking and bending the knee is good, pain or discomfort will limit your activity.
- Take as much weight on the leg as possible.
- You will need to wear the knee splint until day 3 or till you get active leg raise.
- Immediately after surgery commence your circulation exercises (as shown by the physiotherapist).
- From day 1, as pain permits, but must commence by day 3, the following leg exercises a minimum of 2 times a day with 20 repetitions for each exercise.
1. Knee flexion seated

- Sitting, bend and straighten knee.
- Sit on the edge of a table lift lower leg out until the knee is straight.
- Then bend the leg as far as possible underneath the table.
- Maintain this stretched position with the knee bent for 20 seconds. Relax.
2. Straight leg raise

- Lie on your back with the non-operative leg bent so the foot rests on the bed.
- Straighten the knee on your operative leg
- Lift your leg approximately 30cms off the bed (It may take some days before you can do this exercise).
- Keep the knee straight.
- Slowly lower to the bed.
3. Knee extensor quadriceps

- Place a thick rolled up towel under your thigh.
- Pull your toes towards you; lift your heel off the bed until the knee is straight.
- Your thigh should remain resting on the towel.
- Hold for 4 seconds. Relax.
- Repeat 10 times.
4. Knee flexion lying
- Lie on your stomach with both legs straight.
- Bend the knee of the operated leg.
- Feel the stretch in the front of the thigh.
- Do not lift front of the hips off the bed.
Return to Activities After Patellofemoral Arthroplasty
Abstract
Patellofemoral arthroplasty (PFA) is used to treat isolated patellofemoral arthritis, but little is known about post-PFA activity levels and functional outcome scores.

