

Unicompartmental Knee Replacement (UKR)
Unicompartmental knee replacement is a minimally invasive surgery in which only the damaged compartment of the knee is replaced with an implant. It is also called a partial knee replacement. The knee can be divided into three compartments: patellofemoral, the compartment in front of the knee between the knee cap and thigh bone, medial compartment, on the inside portion of the knee, and lateral compartment which is the area on the outside portion of the knee joint.
For The implant we use is the ZUK prosthesis which has the best outcome in the National Joint Replacement Register of the Australian Orthopaedic Association. zimmer.
Traditionally, total knee replacement was commonly indicated for severe osteoarthritis of the knee. In total knee replacement, all worn out or damaged surfaces of the knee joint are removed and replaced with new artificial parts. Partial knee replacement is a surgical option if your arthritis is confined to a single compartment of your knee.
Unicompartmental knee arthroplasty changed dramatically with the onset of minimally invasive surgery. This was popularised primarily in the early 90s by Dr John Repicci. Using the Repicci technique of minimally invasive surgery, it is possible to implant a resurfacing unicompartmental knee replacement as a day surgical procedure. We started doing this procedure in August 1998 after instruction from Dr John Repicci. We have now done over 1,200 of these procedures and approximately 54% of the patients are discharged within 24 hours. This requires a preoperative education program and intense postoperative pain management. The overall satisfaction rate with this procedure is approximately 90% and we expect the survivorship of the implant is approximately 8-10 years. The revision rate of UKRS is approximately 3% per annum translating into a survivorship of 70% by 10 years.
The implant that is currently used is called a Freedom unicompartmental knee replacement that was a modification of the original Repicci prosthesis and is co-designed by Professor Neil. The implant resects minimum bone and therefore can easily be converted to a total knee replacement or revised in the future if necessary. Unicompartmental knee replacement offers the patient with single compartment bone-on-bone knee arthritis the opportunity of improved quality of life with a fairly straightforward procedure for approximately 10 years. We regard it as a pre-knee replacement operation and a way of buying time without he necessity of going through major surgery. Often unicompartmental knee implants feel far more natural than total knee replacements because there is less disruption involved with the surgery and usually far greater range of motion and function. The operation should be performed early in the disease rather than late before other compartments of the knee are involved.
Disease Overview
Arthritis is inflammation of a joint causing pain, swelling (inflammation), and stiffness. Osteoarthritis is the most common form of knee arthritis in which the joint cartilage gradually wears away. It most often affects older people. In a normal joint, articular cartilage allows for smooth movement within the joint, where as in an arthritic knee the cartilage itself becomes thinner or completely absent. In addition, the bones become thicker around the edges of the joint and may form bony “spurs”. All of these factors can cause pain and restricted range of motion in the joint.
Causes
The exact cause is unknown, however there are several factors that are commonly associated with the onset of arthritis and may include:
- Injury or trauma to the joint
- Fractures of the knee joint
- Increased body weight
- Repetitive overuse
- Joint infection
- Inflammation of the joint
- Connective tissue disorders
Symptoms
Arthritis of the knees can cause knee pain, which may increase after activities such as walking, stair climbing, or kneeling.
The joint may become stiff and swollen, limiting the range of motion. Knee deformities such as knock-knees and bow-legs may also occur.
Diagnosis
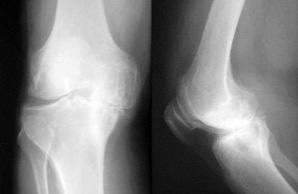
We will diagnose osteoarthritis based on the medical history, physical examination, and X-rays.
X-rays typically show a narrowing of joint space in the arthritic knee.
Prior to Surgery
- You will need to ring the patient liaison nurse from the Day Surgery Unit the day before surgery.
- You will be informed of your admission time for the day of your surgery.
- You will be advised regarding any medications you may be taking.
- You will be given a time from which you need to cease eating and drinking.
What to bring with you?
- Pension / Medicare / Veteran’s affairs cards
- Health insurance details
- X-rays
- You regular medications
- Toiletries
- Clothing (loose fitting)
Day of Surgery
- At your allocated time, you will be admitted to the Day Surgery preoperative area.
- You will be welcomed by the nursing staff and prepared for the procedure.
- Your nurse will ask some questions and record some baseline observations (temperature, pulse, blood pressure).
- You will be asked about any allergies that you may have.
- You will be given some special clothing to put on.
- If you are going home the same day wear some loose-fitting clothes to go home in (i.e. shorts, baggy pants, skirts)
- You will be assisted with the application of some compression stockings (TED stockings). These helps to prevent blood clots forming in the legs and reduce swelling.
- One will be applied to the leg not being operated on. You will need to apply the other to your operated leg on day 3 when you remove your dressing.
Your anaesthetist and surgeon
- In the pre-op area, you will be seen by us.
- We will discuss any relevant medical conditions and history and will insert an intravenous fluid line (drip).
- You may be given some light anaesthesia prior to moving to the operating theatre.
- We will see you and confirm your consent, answer any questions and mark the leg to be operated on.



The operating room
- From preoperative area, you will be transferred on your bed to the operating room.
- You will be assisted onto the operating table.
- Shortly after, your anaesthetist will administer your anaesthetic and you will go to sleep.
- When the anaesthetic has taken effect, you will be positioned on the table and the operation will commence.
Surgical procedure
We may recommend surgery if non-surgical treatment options such as medications, injections, and physical therapy have failed to relieve the symptoms.
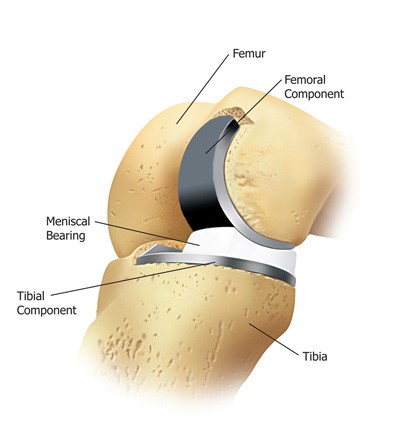
During the surgery, a small incision is made over the knee to expose the knee joint. We will remove only the damaged part of the meniscus and place the implant into the bone by slightly shaping the shin bone and the thigh bone. The plastic component is placed into the new prepared area and is secured with bone cement. Now the damaged part of the femur or thigh bone is removed to accommodate the new metal component which is fixed in place using bone cement. Once the femoral and tibial components are fixed in proper place the knee is taken through a range of movements. The muscles and tendons are then repaired and the incision is closed.
The Partial Knee Procedure
- The procedure is performed in the Day Surgery Unit of St Vincent’s Clinic (Level 3).
- Depending on individual circumstances you may be discharged home 4-6 hours after surgery or you may be required to stay for 1-3 nights in St Vincent’s Private Hospital.
- You will attend an education session about your procedure 1 to 3 days prior to your operation.
- You will require someone at home to assist you for the first three days.
- You will require someone to pick you up to take you home after your surgery.
Advantages of the Partial Knee

- Minimal disturbance to normal knee function
- Less disruption to lifestyle
- Less postoperative pain
- Less bone removed
- Less blood loss
- Less risk of infection, bleeding and wound problems
- Rapid return to normal knee function
- Shorter hospital stay, potentially day only procedure
- Allows for future treatment options (revision)
- Smaller incision
- Feels more like a natural knee
After the procedure
- The surgery takes about 2 hours to complete.
- You will be transferred from the operating room to the recovery unit.
- In recovery, you will be observed and given any pain relief you require. You will stay in the recovery room until you recover from the anaesthetic. I.e. you will be rousable, comfortable and your observations stable.
- This time varies from patient to patient.
Second stage recovery
- Once comfortable you will be transferred to the second stage recovery unit.
- You will be given something light to eat and drink.
- You will notice that you have a large dressing on your operated leg. This dressing extends from your thigh to your toe.
- There will also be a knee immobilizer (splint) in place over the dressing.
Recovery continued

- Under the dressing and resting in the wound, you will have the local anaesthetic catheter and pump. This stays intact until day 3. (See pain buster notes)
- You will also notice the wound drain, which collects any local bleeding from the wound for a couple of hours after the operation. This drain will be removed before you go home.
Before you go home
- Before you go home you may need to take some strong pain tablets (Endone). You will need to take these tablets every 4 hours for the first 2 days after surgery. (See medication notes)
- The physiotherapist will also see you and take you for a walk with crutches or a walker.
Discharge

- You will be able to leave the Day Surgery Unit 4 to 6 hours after your operation.
- You must have someone to collect you from the Day Surgery Unit and take you home.
- You will be given medication to take home and it is very important to take this medication as prescribed.
- You will also receive a dressing pack to change your dressing on day 3.
Your Pain Buster at home
- Your PainBuster pump will remain intact until day 3.
- At home, it should be kept clipped onto the leg bandages or splint to avoid letting it hang or become tangled.
- The balloon shaped pump will slowly deflate as the anaesthetic continues to infiltrate the soft
- tissues in your knee. You will remove this on day 3. (See PainBuster notes)
Your dressing at home
- The thigh to toe dressing needs to remain intact until day 3.
- The knee immobiliser should be worn when walking until the dressing is removed on day 3.
- If showering, you will need to keep your leg dressing dry. A garbage bag and tape is ideal for making it a bit more waterproof.
Day 1 and 2 after surgery

- Remember to rest and keep your leg elevated. 3 or 4 times during the day elevate your leg on pillows and lie flat for 30 minutes.
- Continue to take medication at the prescribed regular intervals.
- Keep to a normal diet and drink plenty of fluids. This will help in the healing process and to maintain normal bowel function.
- When mobilising use your knee splint and crutches. You may weight bear on the operative leg as tolerated.
- You will need to commence your leg exercises a minimum of 2 times / day. (See exercise notes)
- Continue to wear your TED stocking on your non-operated leg.
- Spray liquid ice onto the bandaging around your knee every 2-4 hours until the bottle is empty.
- If the liquid ice runs out before day 3 – start using your ice pack, 4 times a day and keep your leg elevated.
Day 3
- Follow your pain protocol sheet for the first 48 hours after surgery
- You will be mobilising more freely and may not require the knee splint
- Continue with your knee exercises. These are best done 30 minutes after taking your pain medication
- You may now remove and throw away the crepe/tubigrip bandaging
- You may now remove the little op site dressing which is holding the pain buster in place and following this remove the pain buster. You do this by holding a folded piece of white gauze over the skin entrance and gently pulling it out. Apply pressure with the gauze if there is any oozing from the wound.
- DO NOT remove the waterproof dressing which is over the knee wound.
- You may shower and then re-apply a fresh tubigrip + TED stocking
- Start using your ice pack for 30 minutes / 4 times a day with your leg elevated above the level of your heart.
Your dressing

- The Duoderm dressing is water resistant. Please remove the tubi grip and TED stockings for showering.
- It is normal for the Duoderm dressing to become soft and squishy if there is any oozing from the wound.
- If the Duoderm dressing lifts off or rolls up or down, replace it with the spare in your dressing pack and leave it intact until you see us.
Day 4 onwards
- You will need to continue with medications as prescribed.
- Rest/elevation and ice packs 4/day for 30 minutes.
- Wearing your TED stockings.
- Showering as normal.
- When sitting elevate your leg on a stool.
- Exercising your knee as instructed.
Day 10
- At or around day 10 after surgery you will need to see us.
- You will need to have a postoperative x-ray on the same day and visit the physiotherapist to check on your knee movement.
General information
- Bruising around the thigh/knee area is not uncommon and may be a result of the tourniquet used during the surgery. It may extend down the leg as far as the foot. It usually resolved within 10 to 14 days.
- Some swelling and warmth should be expected following surgery.
- If you develop increased redness, swelling or fever, call us or after hours, the hospital or your local doctor.
General expectations
- These are averages, each case is individualised by your general health, age and attitude.
- For approximately 2 weeks after surgery, your activity level is usually limited, however you will be able to walk independently and use bathroom and kitchen facilities.
- After 2 weeks, you will be able to engage in moderate activities such as driving a car and climbing stairs.
- Within 6 weeks you will have resumed most of your normal activities. Squatting and kneeling come with time.
- Complete surgical healing takes 6 to 8 weeks. During this time, some swelling and discomfort is normal and should be manageable with the prescribed medications.
- After this time the knee tissues start to begin to soften and become more natural.
- Some patients may require an injection of cortisone (after 12 weeks) to relieve tissue soreness due to surgery and readjustment of the knee.
- Some patients may experience a small area of numbness on the lateral aspect (outside edge) of the incision. This may or may not resolve over time and can take 6 to 12 months.
Pain Buster notes
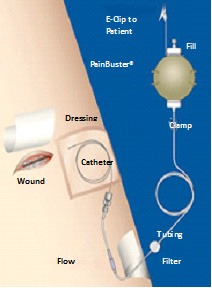
- The Pain Buster pain management system consists of a small round pump filled with local anaesthetic medication.
- The pump is attached to a small catheter (tube) that is placed under the skin close to your incision site.
- The pump automatically delivers the anaesthetic medication at a continual slow flow rate.
- The pump should be pinned to your dressing or clothes whilst in use.
- It is not necessary to squeeze the pump as the balloon deflates as the anaesthetic medication is delivered to the tissues.
- The Pain Buster should be removed with your dressings on day 3.
- The catheter is very small and will be painless to remove at home.
- To remove the pain buster, carefully pull the catheter out in the same direction as it enters your skin.
- There may be a small amount of discharge from the exit point, this is normal.
- A gauze dressing should be placed over the site. This will also be found in your take home dressing pack.
Exercise notes
- To reduce stiffness and obtain maximum function of your knee, it is important to maintain a good balance of rest and exercise.
- Listen to your body; too much activity will produce increased swelling and/or pain; too little activity could prolong your recovery and/or limit your knee mobility.
- Generally walking and bending the knee is good, pain or discomfort will limit your activity.
- Take as much weight on the leg as possible.
- You will need to wear the knee splint until day 3.
- Immediately after surgery commence your circulation exercises (as shown by the physiotherapist).
- From day 1, as pain permits, but must commence by day 3, the following leg exercises a minimum of 2 times a day with 20 repetitions for each exercise.
1. Knee flexion seated

- Sitting, bend and straighten knee.
- Sit on the edge of a table lift lower leg out until the knee is straight.
- Then bend the leg as far as possible underneath the table.
- Maintain this stretched position with the knee bent for 20 seconds. Relax.
2. Straight leg raise

- Lie on your back with the non-operative leg bent so the foot rests on the bed.
- Straighten the knee on your operative leg.
- Lift your leg approximately 30cms off the bed.
- Keep the knee straight.
- Slowly lower to the bed.
3. Knee extensor quadriceps

- Place a thick rolled up towel under your thigh.
- Pull your toes towards you; lift your heel off the bed until the knee is straight.
- Your thigh should remain resting on the towel.
- Hold for 4 seconds. Relax.
- Repeat 10 times.
4. Knee flexion lying
- Lie on your stomach with both legs straight.
- Bend the knee of the operated leg.
- Feel the stretch in the front o the thigh.
- Do not lift front of the hips off the bed.
Post-Operative Care
You may walk with the help of a walker or cane for the first 1-2 weeks after surgery. A physical therapist will advise you on an exercise program to follow for 4 to 6 months to help maintain range of motion and restore your strength. You may perform exercises such as walking, swimming and biking but high impact activities such as jogging should be avoided.
Risks and Complications
Possible risks and complications associated with unicompartmental knee replacement include:
- Knee stiffness
- Infection
- Blood clots (Deep vein thrombosis)
- Nerve and blood vessel damage
- Ligament injuries
- Patella (kneecap) dislocation
- Plastic liner wears out
- Loosening of the implant
What Medications Should I Stop Before Operation?
Many tablets can cause excessive bleeding at operation so it is essential to cease taking the medication well beforehand. However, if you are taking such medication for problems with your heart or blood vessels, please ensure you discuss this with A/Prof Neil or Dr Kalanie.
Stop the following one month (30 days) prior to admission:
- HRT (excluding Prednisone)
- Tamoxifen
- Arava
- Letrozole
Stop the following 5 days prior to admission:
- Alka-Seltzer
- Asasantin
- A.S.A. Aspirin
- Aspirin
- Aspalgin
- Aspro Clear
- Asprodeine Soluble
- Astrix
- Bex
- Bufferin
- Cartia
- Cardiprin
- Clusinol
- Chemgesic
- Codiphen Forte
- Clopidogrel
- Coois
- Codox
- Codral Forte
- Disprin
- Doloxene
- Ectorin
- Ensalate
- Iscover
- Morphalgin
- Orthoxical Cold & Flu Tablets
- Percoden
- Persantin
- Plavix
- Rheumat-ese
- Rhusal
- Solocode
- Solvin
- Solprin
- Salicylamide
- SRA
- Vincents powder/tabs
- Winsprin ANTI-INFLAMMATORY DRUGS
- ACT-3
- Aclin
- Actiprofen
- Advil
- Arthexin
- Arthrotec
- Brufen
- Bugesic
- Candyl
- Celebrex
- Clinoril
- Crysanal
- Dinac
- Doloboid
- Feldene
- Fenac
- Flexin
- Ibuprofen
- Indocid
- Inflam
- Inza
- Mefic
- Methotrexate
- Mobic
- Naprogesic
- Naprosyn
- Nurofen
- Orudis
- Oruvail
- Ponstan
- Priohexal
- Prioxicam
- Proxen
- Rafen
- Rheumacin
- Surgam
- Tilcotil
- Toradol
- Tri-profen
- Arnika
- Echinacea
- Fish Oil
- Garlic (7 Days)
- Ginger
- Ginseng (7 Days)
- Gingko (36 Hours)
- Krill Oil
- Primrose Oil
- Saw Palmetto
- Vitamin E
- Voltaren
ANTICOAGULANTS
Warafin/Coumarin/Marevan cease 5 days pre-op. The tablets will have to be withdrawn prior to surgery and CLEXANE injections are substituted up to the time of operation. ANTICOAGULANT tablets will be resumed after surgery under the direction of Prof Neil.
HERBAL MEDICINE
Arnika, Gingko, Garlic, Echinacea, Fish Oil, Krill Oil, Ginger, Ginseng, Saw Palmetto Vitamin E, Primrose Oil, Krill Oil / Deep Sea Krill Oil
PANADOL, PANADEINE OR PAINKILLERS may be taken for pain relief up to the time of operation.
If you are uncertain about any of your medications please discuss this with A/Prof Neil or Dr Kalanie.
- Outcomes of Unicompartmental Knee Arthroplasty After Aseptic Revision to Total Knee Arthroplasty
- UKR references
All the Patient Forms are Adobe PDF files and require an Adobe Acrobat Reader If you do not have a copy, you can obtain a free copy of the Reader from the Adobe site. Click on the Adobe logo below go download the Adobe Reader.
![]()


