

Computer Assisted Knee Surgery
One of the key factors that determines good clinical and functional results following Total knee replacement surgery is accurate positioning and alignment of components.
Over the last decade it has become increasingly clear that using conventional methods of hand held rods and jigs (still used by 70-80% of surgeons in Australia) to guide positioning of knee replacement components during surgery lacks in accuracy and doesn't allow the surgeon to align the knee correctly in a consistent and reproducible fashion in a high enough percentage of cases. In addition to this, placing rods into the tibia and femoral bone has the added down side of increase pain, blood loss and introducing fat emboli into the blood stream, all which are associated with less than ideal outcome for the patient.
To address these deficiencies, two new methods were introduced: one involves using special infra-red positioning sensors and a computer that work together to assist the surgeon during the operation to accurately perform the bony cuts, forgoing the need for traditional hand held rods and jigs. This first method is often referred to as “computer assisted surgery” (CAS). The computer allows us to accurately cut the correct amount of bone off both the tibia and femur in exactly the right angles to achieve the perfect fit and balance for each patient. This method has consistently been shown to be accurate in a number scientific studies.
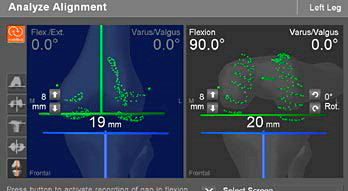
The computer screen shows the surgeon the depth of bony cuts and exact alignment of the prosthesis in real time
The second method relies on manufacturing pre-made cutting guides based on CT or MRI image of the patients own knee prior to the operation. This again forgoes the need to introduce rods into the patient's bones with promise of better prosthetic alignment. This second way is often referred to as "Patient Specific Implant" (PSI) or "Patient Specific Cutting Guides" (PSCG).
Although both systems have been around for now over a decade, they're often used by experienced surgeons in high volume centres. A number of scientific papers have now been published looking at the accuracy of PSI vs CAS and PSI vs Conventional methods. Almost all these papers are showing that Patient specific implants (PSI) fails to correctly position the implants accurately, potentially leading to less than ideal clinical outcome for the patients. (1,2,3,4)
Therefore we've elected to continue using computer assisted surgery which has not only produced very high quality results in our practice but has been shown in scientific literature to be the most consistent manner in ensuring accurate positioning of the Knee prosthesis, which as mentioned earlier, is essential to ensuring a good clinical outcome for the patient.
Materialise's Factory for 3 D Printing Virtual Tour
References:
- Leeuwen, J., Grøgaard, B., Nordsletten, L. and Röhrl, S. (2014). Comparison of planned and achieved implant position in total knee arthroplasty with patient-specific positioning guides. Acta Orthopaedica, 86(2), pp.201-207.
- Lustig, S., Scholes, C., Oussedik, S., Kinzel, V., Coolican, M. and Parker, D. (2013). Unsatisfactory Accuracy as Determined by Computer Navigation of VISIONAIRE Patient-Specific Instrumentation for Total Knee Arthroplasty. The Journal of Arthroplasty, 28(3), pp.469-473.
- Ollivier, M., Tribot-Laspiere, Q., Amzallag, J., Boisrenoult, P., Pujol, N. and Beaufils, P. (2015). Abnormal rate of intraoperative and postoperative implant positioning outliers using “MRI-based patient-specific” compared to “computer assisted” instrumentation in total knee replacement. Knee Surgery, Sports Traumatology, Arthroscopy, 24(11), pp.3441-3447.
- Todesca, A., Garro, L., Penna, M. and Bejui-Hugues, J. (2016). Conventional versus computer-navigated TKA: a prospective randomized study. Knee Surgery, Sports Traumatology, Arthroscopy, 25(6), pp.1778-1783.
- McClelland, J., Webster, K., Ramteke, A. and Feller, J. (2017). Total knee arthroplasty with computer-assisted navigation more closely replicates normal knee biomechanics than conventional surgery. The Knee, 24(3), pp.651-656.
- Rosenberger, R., Hoser, C., Quirbach, S., Attal, R., Hennerbichler, A. and Fink, C. (2007). Improved accuracy of component alignment with the implementation of image-free navigation in total knee arthroplasty. Knee Surgery, Sports Traumatology, Arthroscopy, 16(3), pp.249-257.
All the Patient Forms are Adobe PDF files and require an Adobe Acrobat Reader If you do not have a copy, you can obtain a free copy of the Reader from the Adobe site. Click on the Adobe logo below go download the Adobe Reader.
![]()


